Hirschsprung (HURSH-spruhng) disease is a rare birth defect. Important nerve cells called ganglion cells are normally found in the intestine. When a baby has Hirschsprung disease (or aganglionosis), these cells do not develop while in the womb.
Ganglion cells play a vital role in helping intestines push digested waste (poop) through the bowel. Children with Hirschsprung disease lack some or all of these nerve cells. Stool becomes “stuck” and cannot be passed out of the body.
Most children with Hirschsprung disease are diagnosed shortly after birth or in infancy. Your newborn may delay passing meconium (a dark green poop) within 48 hours (about 2 days) of birth. Other symptoms can include irregular bowel movements, a bloated stomach, or vomiting.
Experts do not know exactly what causes Hirschsprung disease. It may be genetic. It happens more often in boys and can run in families. There is an increased risk of other birth defects.
Why UPMC Children’s?
UPMC Children’s Hospital of Pittsburgh is one of the top pediatric hospitals in the country. We are recognized for excellence in all pediatric specialties. Our gastroenterology and GI surgery program also ranks among the top 10 in the nation.
The Colorectal Center for Children at UPMC Children’s offers expert resources to accurately diagnose, surgically repair, and provide ongoing treatment for children with Hirschsprung disease. Our pediatric specialists provide highly skilled, coordinated, and personalized care. Your care team may include pediatric experts in pediatric surgery, newborn care (neonatology), gastroenterology, genetics, motility, and other specialties.
Does Hirschsprung disease affect all patients in the same way?
The severity of Hirschsprung disease varies. In all cases, healthy nerve cells did not form in the rectum (the end of the colon, before the anus). But these cells can be missing in all or part of the colon and large or small intestine.
- Hirschsprung disease has similar symptoms to other common digestive problems. These include constipation or formula intolerance. Babies may initially respond well to a laxative, suppository, or enema. This can delay diagnosis.
- Mild cases of Hirschsprung disease may not be diagnosed in infants. The most frequent symptom is constipation.
- Moderate to severe cases can lead to proliferative obstructive colitis or enterocolitis. This is a life-threatening condition that needs immediate attention.
The illustrations below highlight the most frequent forms of the disease.
How is Hirschsprung disease diagnosed?
Hirschsprung disease is usually confirmed with a rectal biopsy. In this procedure, a small sample is taken from your child’s rectum. One of our experienced pathologists reviews the tissue to make a diagnosis.
How is the extent of the disease in the colon determined?
| |
Click to enlarge images.
|
|
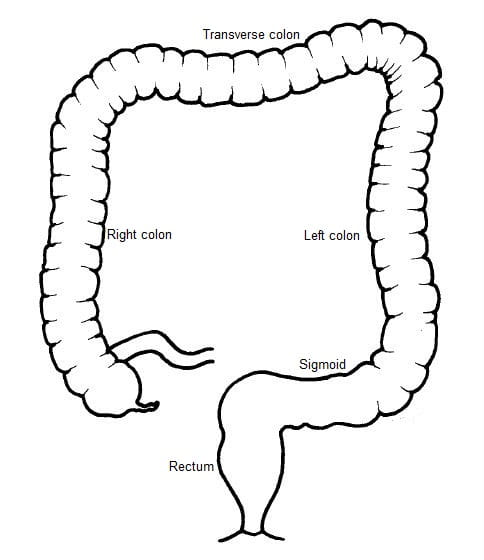
Once your child has been diagnosed with Hirschsprung disease, the next step is a radiological study called a contrast enema. This study shows doctors the structure of the large intestine, colon, and rectum to identify the location of healthy nerve cells.
|

Normal colon |
|
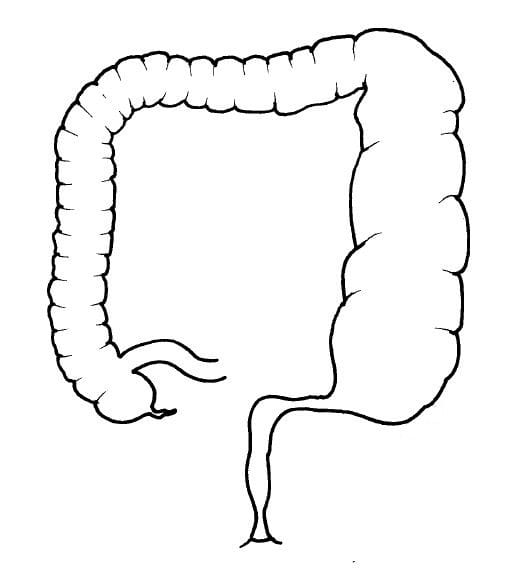
Short-Segment Hirschsprung Disease: Seven of 10 babies born with Hirschsprung disease are missing nerve cells in the rectum making it narrow in size. The part of the colon before the rectum that has normal ganglion cells is enlarged.
|
 Aganglionosis of the rectum Aganglionosis of the rectum |
|
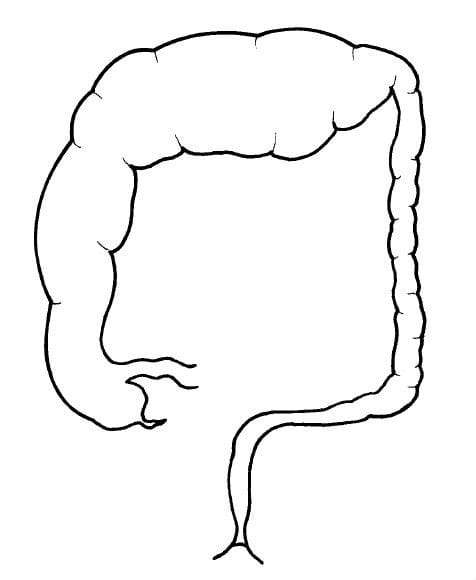
Long-Segment Hirschsprung Disease: One in 5 babies have this form of Hirschsprung disease, where a larger part of the colon is aganglionic (lacking ganglion nerve cells) and narrowed. In this case, the rectum, sigmoid, and left large bowel are missing healthy nerve cells.
|
 Aganglionosis of rectum, sigmoid, and left large bowel (also called a descending colon) Aganglionosis of rectum, sigmoid, and left large bowel (also called a descending colon) |
|
Total Colonic Short-Segment Hirschsprung Disease: In about 1 in 10 babies with Hirschsprung disease, the entire colon is narrow. The small bowel (ileum) is also involved.
|

Total colonic aganglionosis |
How is Hirschsprung disease treated?
Treatment is tailored to your child’s needs.
Stage 1
- Our first goal is to address any bowel obstruction. A rectal catheter is gently inserted into your child’s anus. A warm, mild salt solution washes out built-up stool and gas. The catheter may be in place for several days or longer.
- Some children may need a colostomy before pull-through surgery. This surgical procedure brings a segment of the large intestine out of the body and collects any fecal matter (poop) in an external bag. This is done by creating a temporary opening called a stoma in the abdominal wall. The stoma is then connected to the large or small intestine.
- If the entire colon is missing nerve cells, an ileostomy may be performed. In this procedure, the last segment of the small bowel (the ileum) is brought out onto the surface of the skin to create a stoma.
Stage 2
All children with Hirschsprung disease undergo a pull-through operation to repair the problem. There are different approaches that can be used. Our expert surgeons determine the best solution for your child.
Pull-through surgery is done to:
- Remove the part(s) of the large intestine missing healthy nerve cells.
- Reconnect the healthy part of the intestine with the anus.
Most pull-through surgeries involve the colon. But children with no healthy nerve cells will require a more advanced pull-through procedure.
Stage 3
The final stage is to close your child’s colostomy or ileostomy. Your surgeon may close or take down the stoma at the time of the pull-through surgery or several weeks (or months) later.
What is the prognosis for children with Hirschsprung disease?
Many children with Hirschsprung disease have a normal lifestyle after a pull-through procedure. Some children may need long-term follow up for problems with constipation or fecal incontinence (soiling).
About a third of children who undergo pull-through surgery may at some point show symptoms of intestinal obstruction, called enterocolitis. Symptoms can include constipation, bloating, smelly loose stools, vomiting, and fever. These should be treated immediately. Regularly washing out the rectum to remove any stool also helps reduce the risk of infection. At UPMC Children’s, we help families learn how to administer colonic irrigations.
How can I help if my child has constipation or fecal incontinence?
Our Colorectal Center for Children offers an outpatient Bowel Management Workshop to support children with Hirschsprung disease. We understand the many physical, mental, and emotional challenges they may face. Our compassionate team of experts help them and their family find solutions and relief. They include specialists in surgery, gastroenterology, neurosurgery, psychology, and other fields.
Additionally, our Motility and Neurogastroenterology Center is one of only two pediatric programs in Pennsylvania — and only 15 in the nation. Here, specially trained doctors and support staff help children with complex gastrointestinal and bowel problems. Services include the latest in testing and advanced treatments.