Anorectal malformation (ARM) is a birth defect also known as imperforate anus. It occurs when the baby is growing in the womb, and the anus and rectum do not develop properly. The anus may be missing, closed off, or in the wrong place.
Looking for Anorectal Malformation Care?
On this page
What Is Anorectal Malformation?
Anorectal malformation (ARM) is a birth defect also known as imperforate anus. It occurs when the baby is growing in the womb, and the anus and rectum do not develop properly. The anus may be missing, closed off, or in the wrong place.
How common is anorectal malformation?
Every year, more than a million children worldwide are born with an ARM.
What causes anorectal malformation?
Its cause is unknown.
What are the types of anorectal malformation?
ARM can range from mild to very complex. About one in three children with an ARM has additional health problems.
The illustrations below show the pelvic structures of boys and girls and the most common types of ARM for each.
As you look at the illustrations, note that:
- The colon is also called the large intestine.
- The rectum is the last part of the large intestine.
- The anus is at the end of the rectum, where fecal matter (poop) collects and is released.
- The anal sphincter is made up of two muscle groups — the internal and external muscles — that form a ring around the anus and control bowel movements.
- The anus must exit through the center of the anal sphincter (muscles) to have the best bowel control.
|
Click to enlarge images.
|
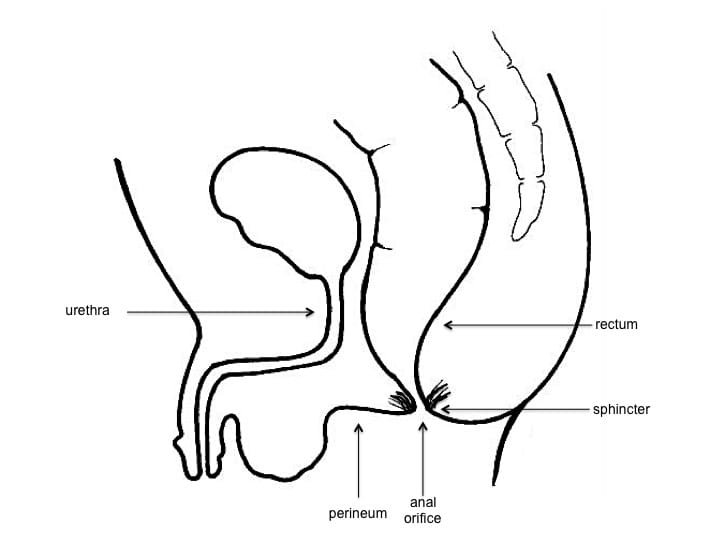
Pelvic Anatomy of a Boy
In boys, the rectum ends in the center of the anal sphincter, forming the anus.
|
 |
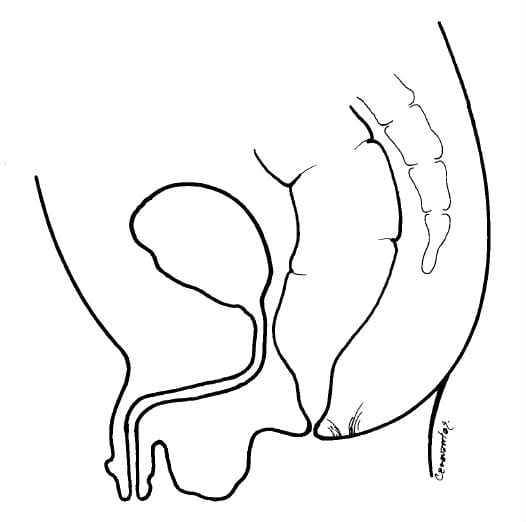
ARM with rectoperineal fistula
The perineum is the area between the anal sphincter and the scrotum (the pouch containing the testicles). An ARM with rectoperineal fistula means the baby has no anus, and the rectum ends in the perineum. outside of the sphincter muscle.
|
 |
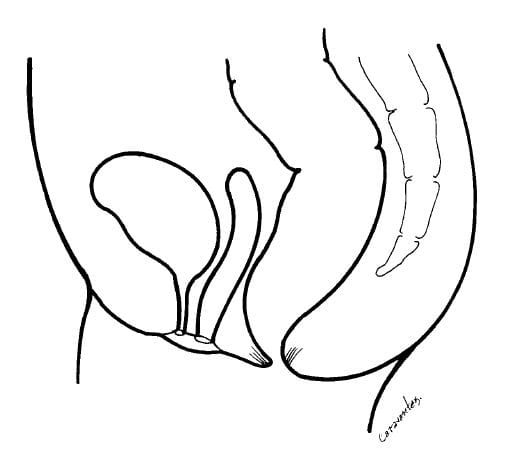
ARM with rectourinary fistula
The urethra and bladder form the lower urinary tract. In this ARM, the baby has no anus, and the rectum ends in any part of the lower urinary tract. Gas and stool may exit through the penis.
|
 |
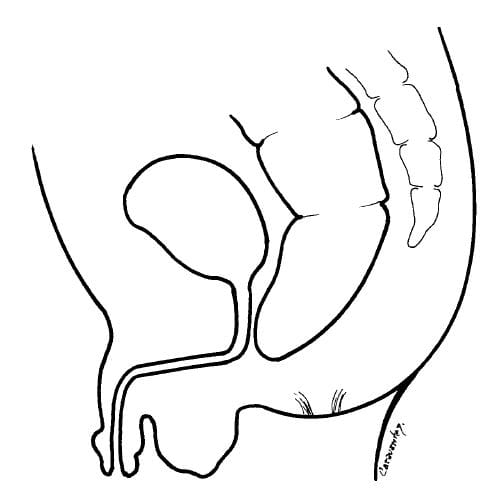
ARM without fistula
In this ARM, the rectum ends in a blind pouch and does not connect to the outside or the urinary tract.
|
 |
|
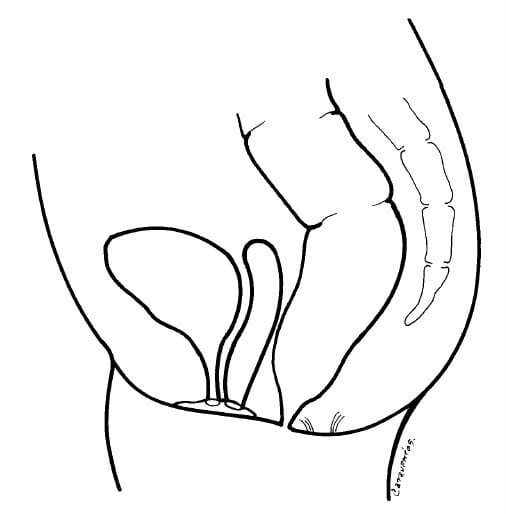
Pelvic Anatomy of a Girl
In girls, the rectum also ends in the center of the anal sphincter, forming the anus. The vagina is located in front of the rectum.
|
 |
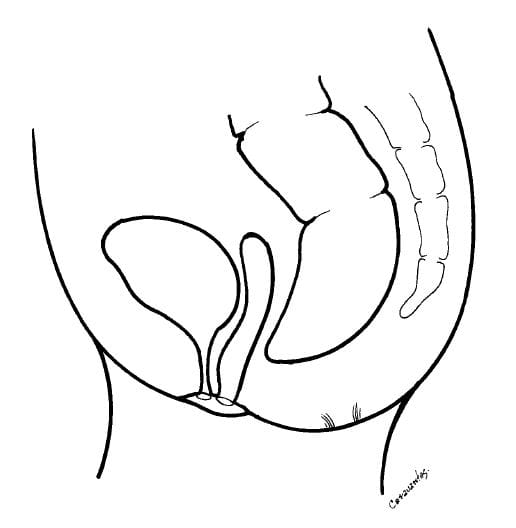
ARM with rectoperineal fistula
The perineum is the area between the anal sphincter and the vulva, the external opening of the vagina. In this condition, a girl does not have an anus, and the rectum ends in the perineum outside the sphincter muscles.
|
 |
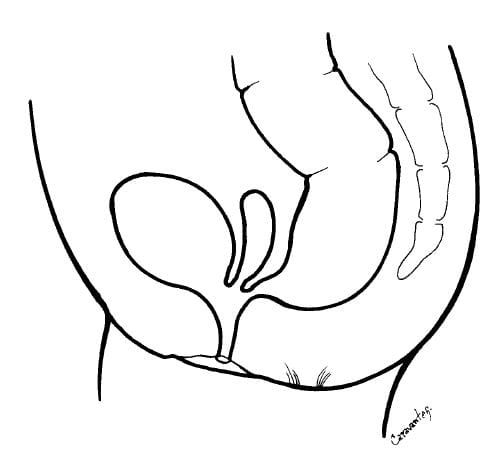
ARM with rectovestibular fistula
This is the most common type of ARM in girls. In this condition, a girl does not have an anus, and the rectum abnormally connects near the entrance of the vagina (the vaginal vestibule). It causes gas and feces to exit the vaginal vestibule. This ARM is often misdiagnosed as rectovaginal fistula.
|
 |
ARM without fistula
In some girls, the rectum ends in a blind pouch and does not connect to the outside or the vaginal vestibule. This is known as ARM without fistula.
|
 |
Cloaca anomaly
Cloaca anomaly is a rare ARM where the rectum, vagina, and urethra fuse together instead of separating. There is only a single opening instead of three.
|
 |
Back to top
How Do You Diagnose Anorectal Malformations?
The most frequent types of ARMs are typically diagnosed during a newborn’s initial physical exam or if a baby doesn’t have a bowel movement within 48 hours (about two days) after birth.
Back to top
How Do You Treat Anorectal Malformations?
All children with ARMs must undergo an operation called anorectoplasty or pull-through surgery. The goal of this operation is to repair the malformation and bring the rectum to the outside of the body through the center of the anal sphincter.
Children with more complex ARMs may require multiple surgeries performed over a period of time, starting with a colostomy. This surgical procedure brings a segment of the large intestine out of the body and collects any fecal matter (poop) in an external bag. This is done by creating a temporary opening called a stoma in the abdominal wall. The colostomy is often closed a few months after pull-through surgery.
What care is needed after pull-through surgery?
The pull-through wound should be kept clean and dry. Two weeks after surgery, anorectal dilatations will begin to keep the anus a normal size and prevent it from narrowing or closing. Your pediatric surgeon or nurse will teach you this simple procedure.
What is the prognosis for intestinal function and fecal continence after pull-through surgery?
The outlook depends on the type and complexity of your baby’s ARM and any associated birth defects. For example, about one in four children with an ARM will experience fecal incontinence (uncontrolled bowel movements).
Your child will need long-term follow-up to detect and treat any of these problems in a timely way:
Back to top
Why Choose UPMC for Anorectal Malformation Care?
UPMC Children’s Hospital of Pittsburgh is one of the top pediatric hospitals in the country. We are recognized for excellence in all pediatric specialties. Our gastroenterology and GI surgery program also ranks among the top 10 in the nation.
- The Colorectal Center for Children at UPMC Children’s offers comprehensive treatment and compassionate support for children with an ARM and their families. Our pediatric surgeons and specialists will provide highly skilled, coordinated, and personalized care.
- In addition to a pediatric surgeon, your care team may include experts in pediatric gastroenterology, urology, gynecology, and other specialties.
Back to top